
by Andrea L., GRM Deputy Director & Chief Program Officer
Franklin Foer’s book, How Soccer Explains the World (2004), and David Winner’s, Brilliant Orange (2000), look at the relationship between a team’s style of play and how it reflects culture and socioeconomic conditions in a country. Watching the 2023 Women’s World Cup with my daughter, I can’t help but smile through the games. Each team looks different, plays differently, and has different communication styles—all reflections of who we are as nations and as people. And while the differences may be striking at first, what underlies them is the incredible work ethic it takes to become a professional athlete, the grit it takes to battle it out for 90 minutes at full speed, the maturity to perform on the world stage with millions of people scrutinizing your every move, the confidence to be a leader both on the field and off.
What most people don’t know is that a significant portion of GRM business is conducted on the sidelines of soccer fields. If you’re talking or messaging with me on weekday evenings or on the weekend, chances are I am either pacing the field or sitting in my camping chair watching my daughter play. As in the above books, her style of play on the field directly reflects who she is as a person and our values as a family.
Raising a girl is different than raising a boy. Each has a unique way of interacting with the world, and more importantly, how the world interacts with them. I remember in my late teens telling my aunt that I wasn’t a feminist. Her response? “You don’t have to be because I was. You’re welcome.” Ouch. I sat down and shut TF up.
We’ve come a long way in just over 100 years. From women receiving the right to vote during my grandmother’s generation to my aunt attending university, but only having a choice of three careers—nurse, social worker, or teacher—to me, feeling like I didn’t need to be a feminist but still witnessing rampant sexual harassment in the workplace (no, not someone telling a female colleague that they look nice, I mean unwanted physical contact and threats). Now, my daughter, who plays on both a girls’ travel soccer team and a co-ed team where she kicks ass as a defender and then sticks out a hand to help someone up after a tackle. She thinks nothing of their gender differences other than the age-appropriate, “Sixth-grade boys are so annoying!”
In both Ukraine and Iraq, GRM’s programs have deliverables that empower women through education and leadership. Some people push back against this and feel we are disempowering men or have a biased approach. Why should women be prioritized in medical training efforts? Why should patient care take extra consideration with female patients? Why do we need to be aware of sending both men and women surgeons, physicians, medics, and nurses to needed areas?
Well, because of reality. In many of the places we work, the female-to-male nurse ratio is about 70% women and 30% men. However, the nursing leadership ratio is 0% women to 100% men. Yikes. And during disasters and conflict, women and children are vulnerable to sexual and gender-based violence disproportionately to men. So, we ask extra questions. We spend extra time in patient care to make sure there isn’t a hidden wound. We model professional collaboration between men and women. We try to include balanced ratios in training efforts. We aren’t prioritizing based on gender, but instead acknowledging that we exist in equal ratios as humans on this planet (approximately 101 men to every 100 women) and try to reflect that in our efforts. We do it so hopefully the next generation doesn’t have to.
Watching the Denmark/China Women’s World Cup game while I write this, I think about the first time I understood “strong was the new pretty” for our girls. My daughter was 4 years old, and we were at a classmate’s birthday party. She was the only girl invited, and all the parents stood around while the kids swung at the piñata hanging from a tree. The expectation bar was low and we cheered anytime a kid made contact.
My daughter was last in the rotation, letting other kids go before her and cheering for her friends. When it was her turn, she stepped up to the piñata and swung the stick so hard and with such control that it hit smack in the center of the donkey piñata and the whole thing burst apart, sending candy flying in all directions. Every father at the party audibly gasped and turned to stare at me with their mouths hanging open. My daughter looked back at me and smiled, then helped a boy with a casted broken arm gather up candy for his bag.















 Above: Dr. Dairon Elisondo Rojas, a Critical Care Physician originally from Cuba, who worked as a
Above: Dr. Dairon Elisondo Rojas, a Critical Care Physician originally from Cuba, who worked as a
 Above 1: Several of GRM’s wonderful local team during the early days of clinic work in the camp.
Above 1: Several of GRM’s wonderful local team during the early days of clinic work in the camp.

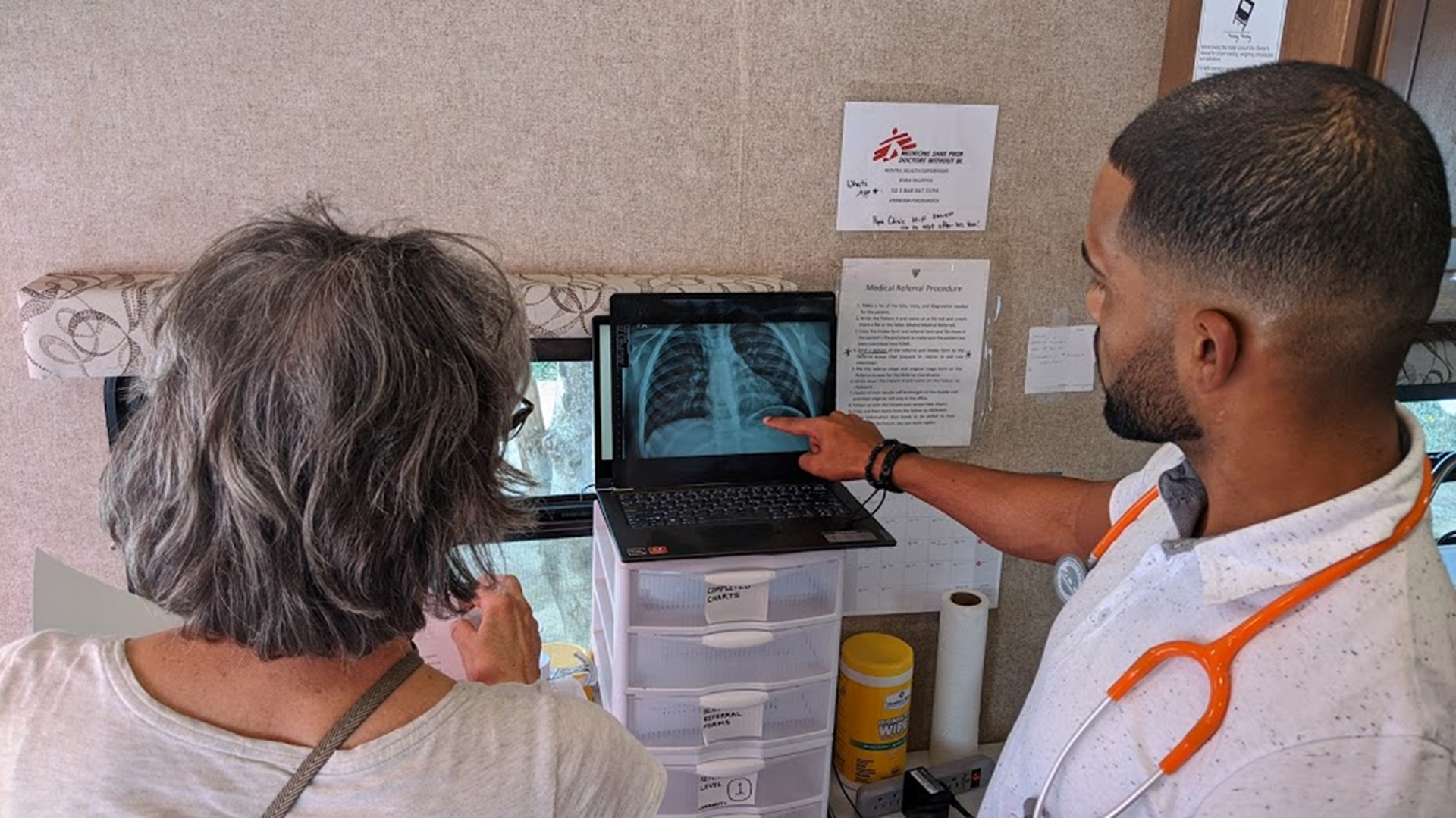
 Above: GRM’s Mobile Clinic, where staff and volunteers treated patients when the asylum-seekers’ encampment still existed.
Above: GRM’s Mobile Clinic, where staff and volunteers treated patients when the asylum-seekers’ encampment still existed.
 Above 1: Mark McDonald, GRM’s Matamoros Project Manager from 2021 to 2022. In 2022, Mark was promoted to GRM’s Director of Strategic and Operational Integration.
Above 1: Mark McDonald, GRM’s Matamoros Project Manager from 2021 to 2022. In 2022, Mark was promoted to GRM’s Director of Strategic and Operational Integration.


 Above: Group pictures with more of GRM’s incredible staff, volunteers, partners and local team members who worked tirelessly in Matamoros over the years.
Above: Group pictures with more of GRM’s incredible staff, volunteers, partners and local team members who worked tirelessly in Matamoros over the years. Last Friday, GRM encountered a Haitian refugee living in the Senda de Vida Shelter, who was 28 weeks pregnant and presenting with a medical condition called pre-term premature rupture of the membranes (PPROM), meaning her water broke too early. This condition is dangerous for the mother due to high risk of infection and high probability of emergency cesarean section. It is also dangerous for the premature baby, whose lungs are not fully developed and will need NICU care immediately after delivery.
Last Friday, GRM encountered a Haitian refugee living in the Senda de Vida Shelter, who was 28 weeks pregnant and presenting with a medical condition called pre-term premature rupture of the membranes (PPROM), meaning her water broke too early. This condition is dangerous for the mother due to high risk of infection and high probability of emergency cesarean section. It is also dangerous for the premature baby, whose lungs are not fully developed and will need NICU care immediately after delivery.
 At the hospital, the patient was immediately transferred through the ER and into the Labor and Delivery Unit. The L&D staff were pleased to hear the patient had already received antibiotics and a steroid injection at the GRM Clinic, noting GRM’s quick thinking and fast action potentially helped the patient avoid an emergency premature c-section, and certainly helped prevent infection or worse complications.
At the hospital, the patient was immediately transferred through the ER and into the Labor and Delivery Unit. The L&D staff were pleased to hear the patient had already received antibiotics and a steroid injection at the GRM Clinic, noting GRM’s quick thinking and fast action potentially helped the patient avoid an emergency premature c-section, and certainly helped prevent infection or worse complications.
 Louvens (pictured right with Kirby), is on GRM’s Team Reynosa and serves as a translator. Louvens was born in Haiti and traveled to the Dominican Republic when he was 5 years old. At 27, he saved up enough money to move to Brazil, where he lived for seven years working to save up more money and begin his travel to America. At the age of 34, he started his three-year journey to Reynosa.
Louvens (pictured right with Kirby), is on GRM’s Team Reynosa and serves as a translator. Louvens was born in Haiti and traveled to the Dominican Republic when he was 5 years old. At 27, he saved up enough money to move to Brazil, where he lived for seven years working to save up more money and begin his travel to America. At the age of 34, he started his three-year journey to Reynosa.